Treatments & Services
Gynecologic Cancer Treatments | Robotic Surgery, Chemotherapy & more

HIPEC in Gynecological Oncology (Hyperthermic Intraperitoneal Chemotherapy)
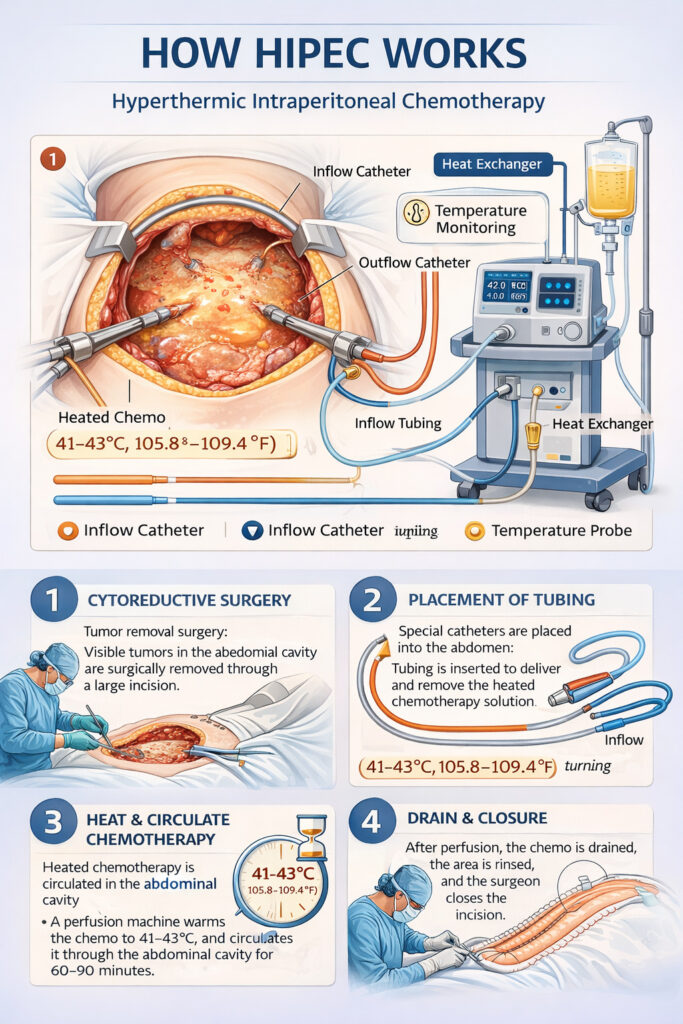
HIPEC is a specialized treatment in which heated chemotherapy is circulated in the peritoneal cavity immediately after cytoreductive surgery (CRS) to destroy microscopic residual cancer. It is increasingly used in gynecologic malignancies, especially ovarian cancer.
1. Rationale / Principle
- Many gynecologic cancers (especially ovarian) spread within the peritoneal cavity
- HIPEC delivers high concentrations of chemotherapy locally with minimal systemic toxicity
- Heat (41–43°C) enhances drug penetration, increases tumor cell death, and potentiates chemotherapy activity
- Aims to kill microscopic residual disease after maximal cytoreduction (CC-0/CC-1)
2. Mechanism of Action
Role of hyperthermia
- Increases cell membrane permeability
- Induces protein denaturation
- Enhances cytotoxicity of many drugs
- Selectively affects malignant cells more than normal tissue
Chemotherapy effect
- High intraperitoneal concentration
- Reduced systemic absorption → fewer systemic side effects
- Longer tumor exposure time
3. Indications in Gynecologic Oncology
a) Ovarian Cancer (Major Indication)
1. Primary advanced ovarian cancer
- Stage III disease after interval cytoreduction (post-NACT)
- Supported by the OVHIPEC-1 trial, showing improved recurrence-free and overall survival when HIPEC with cisplatin was added to interval debulking.
2. Recurrent ovarian cancer
- Considered for platinum-sensitive recurrent disease undergoing secondary cytoreduction
- Data evolving; used in specialized centers
b) Endometrial Cancer
- Very limited role
- Only considered in highly selected patients with peritoneal carcinomatosis
4. Common Chemotherapeutic Agents Used
- Cisplatin (most common)
- Paclitaxel
- Doxorubicin
- Mitomycin-C
Typical parameters
- Temperature: 41–43°C
- Duration: 60–90 minutes
- Perfusion volume: 2–3 L
- Open (“Coliseum”) or closed technique
5. Advantages of HIPEC
- Targets microscopic residual disease after surgery
- Higher local drug concentration with lower systemic toxicity
- Hyperthermia improves drug uptake
- May improve PFS and OS in selected ovarian cancer patients
- Reduces risk of peritoneal recurrence
6. Limitations
- Requires highly skilled CRS surgery and specialized equipment
- High perioperative morbidity if cytoreduction is extensive
- Long operative time
- Not suitable for non-operable or bulky residual disease
- Evidence strong for interval debulking but still evolving for primary upfront surgery or recurrence
7. Morbidity / Complications
- Renal toxicity (especially cisplatin → requires vigorous hydration)
- Bone marrow suppression
- Anastomotic leak
- Infection, sepsis
- Electrolyte imbalance
- Thermal injury (rare)
8. Contraindications
- Poor performance status
- Extra-abdominal metastasis (liver parenchymal, lung, brain)
- Incomplete cytoreduction (residual tumor >2.5 mm)
- Severe renal dysfunction
- Extensive mesenteric involvement (prevents bowel reconstruction)
9. Evidence Summary
OVHIPEC-1 Trial (2018)
- HIPEC + Interval Cytoreduction showed:
- ↑ Progression-free survival
- ↑ Overall survival
- No increase in major morbidity
Ongoing Trials
- OVHIPEC-2 (role in primary upfront surgery)
- Trials in recurrence and other cancers
10. Current Role
HIPEC is not standard for all patients, but is recommended for:
- Stage III ovarian cancer undergoing interval cytoreductive surgery
- Select cases of recurrent ovarian cancer
- Rarely, metastatic endometrial or cervical cancer with peritoneal spread
Usually carried out only in high-volume tertiary cancer centers.
Need a consultation? Contact us to know our availability and contact details.

Dr Richa Bansal
Dr. Richa Bansal MBBS, MS (Obstetrician and Gynecologist), DNB, MCh Gynecological Oncology (Tata Memorial Hospital, Mumbai) is a Sr. Consultant Gynecological Onco Surgeon, Laparoscopic & Robotic Surgeon
What we say?
What our patients say?
Image Gallery